Thyroid Nodules
What is a thyroid nodule?
A thyroid nodule is a growth of thyroid tissue within the thyroid gland. It may or may not produce a clinically visible lump or can be felt as a lump on the front of the neck. Thyroid nodules rarely impact thyroid function.
Thyroid nodules are common. Approximately 4% of the general population harbors clinically detectable thyroid nodules, and there is a high prevalence of thyroid nodules in iodine-deficient countries.
Most of the thyroid nodules are non-cancerous. However, the main concern is to determine whether the thyroid nodule is benign (non-cancerous) or malignant (cancerous).

 The thyroid gland is butterfly-shaped in the lower part of your neck, in front of your windpipe. It has two lobes: the right lobe and the left lobe. A narrow isthmus joins the right and left lobes.
The thyroid gland is butterfly-shaped in the lower part of your neck, in front of your windpipe. It has two lobes: the right lobe and the left lobe. A narrow isthmus joins the right and left lobes.
The thyroid gland mainly comprises two types of cells: thyroid follicle cells and C cells. The thyroid follicular cells produce thyroid hormones secreted into the blood circulation and regulate the function of every cell and tissue. Your thyroid produces thyroxine (T4) and triiodothyronine (T3), necessary for good health and control of your metabolism and energy levels. C cells produce calcitonin, which helps to regulate calcium metabolism.
The hypothalamus and pituitary gland in your brain regulate T4 and T3 production. When T4 and T3 levels are low, the hypothalamus produces thyrotropin-releasing hormone (TRH) to signal the pituitary gland to produce thyroid-stimulating hormone (TSH). The TSH travels in the bloodstream and signals the thyroid gland to produce more T4 and T3. When T4 and T3 levels are high, the pituitary gland stops producing TSH.
- Solid thyroid nodules – these nodules account for most thyroid nodules.
- Thyroid cysts—these nodules contain liquid inside and are usually benign. They typically do not impact thyroid function. When they are causing discomfort, they can be drained with a needle, surgically removed, ablated, or removed using minimally invasive techniques.
- Overactive ‘toxic’ thyroid nodules: Only a minority of thyroid nodules make extra thyroid hormone, called “toxic adenomas .”Toxic adenomas are usually benign, and the options for treating these are like other causes of hyperthyroidism.
The cause of most benign nodules is unknown, but they are often found in members of the same family. Worldwide, the diet’s lack of iodine is a common cause of nodules. Thyroid nodules become more common with increasing age, and women are more likely to have them than men.
Most of the thyroid nodules do not typically cause any symptoms.
Large nodules can press on the structures within the neck to cause:
- Discomfort pain or pressure on the front of the neck
- Difficulty in breathing
- Difficulty in swallowing
- Voice changes, especially hoarseness of voice
Some nodules can cause symptoms like hyperthyroidism – racing of heart, heat intolerance, etc.
Most of the time, these nodules are identified when you go for a radiological exam (e.g., X-ray or CT scan of the neck) and are not related, especially to the thyroid gland.
Dr Reena Thomas will help diagnose this condition by doing a comprehensive medical evaluation and physical examination of your neck. She will order blood tests to screen for thyroid function abnormalities.
She will perform an ultrasound of the neck in her office to get an exact picture of the thyroid gland and to characterize the nodule—solid, cystic (fluid-filled), or mixed. She will also be able to observe if there are any abnormal lymph nodes in the neck.
Depending on the size and characteristics of the nodules, she may refer you for a CT scan of the neck without contrast to find out if there is compression of the windpipe or important structures of the neck.
Most benign nodules do not need a biopsy or surgery. Thyroid nodules are generally monitored with an ultrasound of the neck at regular intervals, depending on their size, location, and characteristics.
Thyroid nodules that are larger than 1.5 cm or have ultrasound characteristics that are suspicious of cancer are biopsied to screen for cancer.
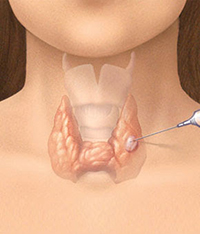
Fine needle aspiration biopsy (FNA) of thyroid nodule
Dr. Reena Thomas will decide on which thyroid nodules require a fine needle aspiration biopsy to screen for cancer after performing a comprehensive ultrasound examination of your neck in her office.
Fine needle aspiration biopsy (FNA) of the thyroid nodule is a procedure in which cells or tissues are collected from the body for further analysis. A pathologist will examine the sample to determine whether it contains cancerous cells.
FNA of the thyroid nodule is done using ultrasound guidance from Dr. Thomas in the office. A small tissue sample is removed from the thyroid nodule using a small, thin, fine-gauge needle that is smaller in diameter than the needle used in most blood draws. Medications (1% lidocaine and ethyl chloride spray) are used to numb the area before the biopsy. The sample is sent to the pathology lab for analysis following the FNA. Once the results are available, Dr. Thomas will communicate them to you personally and discuss further management.
Depending on the results, she will coordinate further management with the endocrine surgeon (if you need surgery). If needed after surgery, she will refer you for radioiodine therapy to a nuclear medicine specialist. In advanced or aggressive thyroid cancer, you will be referred to an oncologist.
Long-term follow-up is determined by the size and characteristics of the thyroid nodules. Smaller thyroid nodules do not need any follow-up. However, larger nodules or nodules causing symptoms and having suspicious characteristics will need monitoring with an ultrasound of the neck at regular intervals.
Thyroid nodules require careful evaluation to rule out the presence of cancer. Dr. Reena Thomas, a board-certified endocrinologist in Southern Maryland, provides expert diagnosis and management of thyroid nodules in Prince Frederick and Annapolis. Contact us today to schedule an evaluation and receive personalized endocrine care.
At a Glance
Dr. Reena Thomas, MD
- Dual American board-certified endocrinologist
- Author of numerous academic and clinic research
- Learn more